



Pregnancy and Vaccination
Maternal deaths increase, no robust safety data, but do it anyway.


The push to get a needle in every arm goes further than mRNA for COVID. While vaccinating during pregnancy has occurred for many decades on a small scale, the relatively recent push to vaccinate pregnant women is alarming at best. Pushing the COVID injection on pregnant women was and is indicative of the laissez-faire attitude toward safety and the imbedded and arrogant attitude that all vaccination is ‘safe and effective’ even though mRNA is a new technology, and more gene therapy than vaccine. A recent article (linked below) conveys the rise in maternal deaths across ethnicities in the US. One look at the Excipient list of all vaccinations administered in the US would give rise to doubt and pay careful attention to the vaccines administered to a pregnant woman: TDaP, Flu vax, COVID (do we know all the ingredients yet? Informed consent anyone??) and more recently RSV vaccine. According to this study, no safety concerns as reported, but a recent article in Salon reports otherwise where safety IS a concern in this and other studies regarding RSV.
The excipient list above shows us that the TDaP vaccine contains:
Glutaraldehyde is an organic compound with the formula (CH2)3(CHO)2. The molecule consists of a five carbon chain doubly terminated with formyl (CHO) groups. It is usually used as a solution in water, and such solutions exists as a collection of hydrates, cyclic derivatives, and condensation products, several of which interconvert. Because the molecule has two carbonyl group that are reactive to primary amine groups (even as its hydrates), it can function as a crosslinking agent for any substance with primary amine groups and develop imine connected links. Crosslinking rigidifies and deactivates many biological functions, so in this way, glutaraldehyde solutions are used as biocides and as fixative. It is sold under the brandname Cidex and Glutaral.[3][4][5][6] As a disinfectant, it is used to sterilize surgical instruments.[3]
Uses
Biochemistry
Glutaraldehyde is used in biochemistry applications as an amine-reactive homobifunctional crosslinker and fixative.[7][8] It kills cells quickly by crosslinking their proteins. It is usually employed alone or mixed with formaldehyde[9] as the first of two fixative processes to stabilize specimens such as bacteria, plant material, and human cells. A second fixative procedure uses osmium tetroxide to crosslink and stabilize cell and organelle membrane lipids.Another application for treatment of proteins with glutaraldehyde is the inactivation of bacterial toxins to generate toxoid vaccines, e.g., the pertussis (whooping cough) toxoid component in the Boostrix Tdapvaccine produced by GlaxoSmithKline.[10]
That is ONE toxin in this vaccine and ONE vaccine they administer to pregnant women.
From the Salon article:
”GlaxoSmithKline (GSK) last year stopped a late-stage clinical trial of its RSV vaccine in pregnant people over an elevated risk of premature birth and associated neonatal deaths in the babies born prematurely. In the GSK trial, premature birth was 38% more likely in the vaccinated pregnancies than in the placebo group. And there were hints of excess premature births as well in Pfizer’s data presented to the panel yesterday. The FDA advisers expressed frustration that the company’s final phase 3 trial wasn’t large enough to know whether the increased rate in the vaccinated group compared with the placebo group—5.7% versus 4.7%—was a real effect as the difference wasn’t statistically significant.”
It’s concerning that maternal deaths took a considerable jump around 2005. Interesting that this is when the WHO began pushing to vaccinate for the flu during pregnancy.
“The WHO has recommended influenza vaccination during influenza season for all pregnant women since 2005; however, most European countries introduced seasonal influenza vaccination for pregnant women only after the H1N1/09 influenza pandemic.”
Vaccines given to pregnant women have not been proven safe regardless of what CDC, Mayo Clinic or PubMed says. I find the literature lacking in anything contrary to “vaccines are safe and effective” regardless of the demographic which leads me to believe that the literature is extremely biased FOR the use of vaccines and rarely if ever report on real issues with vaccinating while pregnant, an infant, or otherwise.
Here is the article.
https://www.statista.com/chart/2231/maternal-mortality-rate/
This article states possible reasons for increased maternal mortality, for example there are more older women having babies now, but when stratified for age, rates of death were the highest in 20-24 age groups.
 United States 25 Developed Regions 20 15 10 5 Maternal Mortality Ratio 1990 2013 380 210 26 16 430 230 12 28 1990 World Developed Regions Developing Regions United States 1995 -45% -38% -47% +136% 2000 Source: World Health Organization 2005 2013 Mashable statista'")
Pregnancy down regulates cellular immunity so the body relies on humoral immunity. Then they stimulate it with vaccines. No real safety has occurred, just post vaccination monitoring of disease in which they flout any adverse outcomes and push false ideas of reduced disease rates. Like tetanus vax. This study done in 1961 in New Guinea illustrates this point. Go to page 787 under Results. The study looked at all infants born with vaccinated mothers and followed the infants for 2 weeks after birth and only looked at deaths from tetanus.

Want to reduce tetanus after birth? Use clean utensils and wash hands. Remember when washing hands was scoffed by the medical community? They are literally killing ppl with these policies.
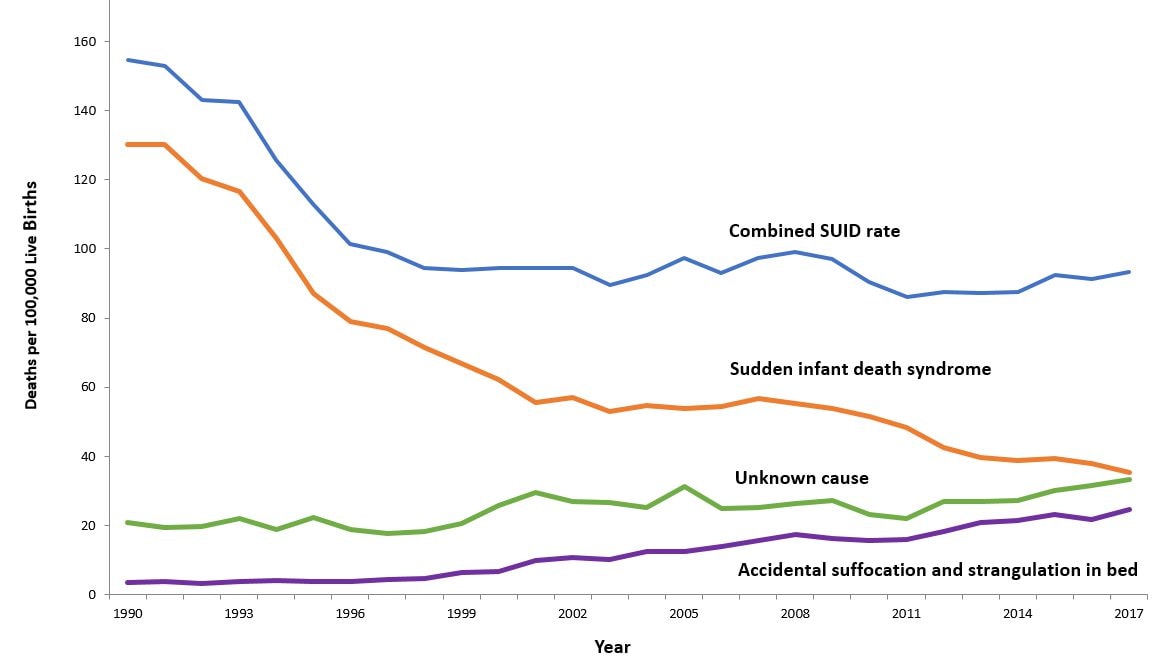
A decrease in infant mortality rates slowed after an uptick of the HEP B at birth where historically we saw major drops in infant mortality. Hep B vaccine injections in new borns began in 1991, but by 2002 CDC changed it’s inclusion criteria for new borns receiving the injection from “at birth or 1-2 months after birth” to “before discharge”, and again in 2005 to “all new borns” including some premature new born weighing “4.4 pounds or more”. Of course CDC et al attribute vaccines to a decrease in infant mortality, but many of us know it is a much more complicated issue that communicable disease that caused infant mortality. Many factors come into play including nutritional status, hygiene, and basic knowledge of birthing. I do wonder what the mortality rate was prior to modern medicine, say in the Native American population before we imposed our ways onto them. The CDC still thinks it can eradicate viruses with vaccines, a feudal attempt at combatting nature, which time and time again backfires. When will humans learn they cannot control nature.

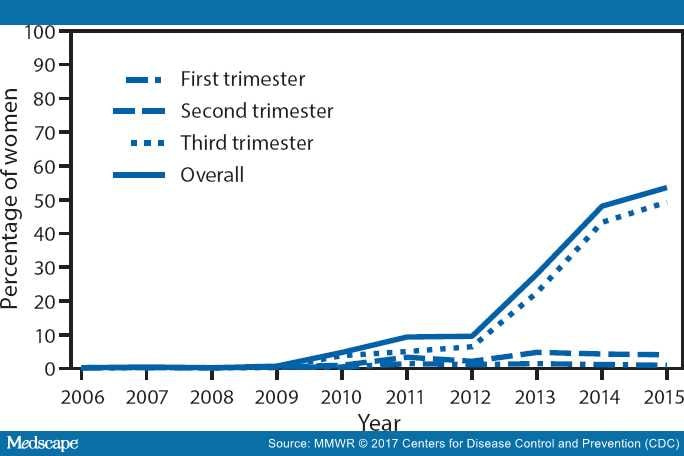
The graph above shows TDaP Coverage in the US. 2006 to 2015.
Here is more recent study than the one listed above completed in 1961 on Tetanus vaccination. From the study: “Even before tetanus vaccine was available, neonatal tetanus became increasingly rare in most of Europe and North America through hygienic childbirth practices and cord care.” This study also cites the New Guinea study, the one referenced above that did not assess safety. Also from the study: “Studies in Africa and Asia show that interventions to improve education and birth hygiene have a substantial effect on maternal and neonatal tetanus, even without vaccination programmes.”
Of course the establishment contributes the decline in neonatal and maternal tetanus to vaccination, but the WHOs attempt at ‘eradication’ of tetanus included hygiene and surveillance as well. So could we say it’s the vaccine? The MOST anyone could say is it MAY have contributed. But where are the safety studies?
So, on to maternal mortality……

According to the WHO, here are the reasons some women die worldwide within a year of giving birth. Some could be attributed to obesity and poor diets, but all these blood clotting issues and infection issues potentially point at immune issues. Vaccinating during pregnancy is certainly something to consider when evaluating these deaths considering infections is listed as a major cause of death.
Severe bleeding (sometimes called hemorrhage)
Infections
Blood pressure disorders of pregnancy, including preeclampsia and eclampsia
Complications of labor and delivery
Unsafe abortion
According to the CDC this is why some women die in the US:
In the United States, the main causes of pregnancy-related deaths include the following:
Severe bleeding (sometimes called hemorrhage)
Infections and sepsis
Cardiovascular conditions, such as:
Blockages (sometimes called embolisms) in arteries and veins
Stroke (also called cerebrovascular accidents)
Blood pressure disorders of pregnancy, including preeclampsia and eclampsia
Heart muscle problems (called cardiomyopathy)
Heart disease
Problems with anesthesia
Amniotic fluid embolism
Non-cardiovascular conditions, such as diabetes and breathing problems
Pertussis Vaccination
A quick PuMed search lended me this systematic review of the literature regarding pertussis vaccination during pregnancy. These are the results:
“We identified 1273 articles and included 22 studies (14 for safety; 8 for effectiveness), comprising 1.4 million pregnant women in safety studies and 855,546 mother-infant-pairs in effectiveness studies. No significant differences between vaccinated and unvaccinated women and their infants were observed for safety outcomes with the exception of fever and chorioamnionitis. Compared to no vaccination, three studies showed a significantly increased relative risk for the presence of the ICD-9 code for chorioamnionitis in electronic patient data after pertussis vaccination. However, no study reported an increased risk for clinical sequelae of chorioamnionitis after vaccination during pregnancy, such as preterm birth or neonatal intensive care unit admission. Vaccine effectiveness against pertussis in infants of immunized mothers ranged from 69 to 91% for pertussis prevention, from 91 to 94% for prevention of hospitalization and was 95% for prevention of death due to pertussis. Risk of bias was serious to critical for safety outcomes and moderate to serious for effectiveness outcomes. GRADE evidence quality was moderate to very low, depending on outcome.”
The problem with safety studies and pregnancy is glaring. Studies either assess for only birth defects. Many only assess safety up until birth, some go 14 days. What’s more is this evidence straight from the WHO and their Global Vaccine Safety Summit, that safety studies are not robust in regards to vaccination and pregnancy. Starts at 1:09.
This study titled “Global Perspectives on Immunization During Pregnancy and Priorities for Future Research and Development: An International Consensus Statement” conveyed this in the Abstract section: “Although there is increasing evidence to support vaccination in pregnancy, important gaps in knowledge still exist and need to be addressed by future studies.”
Furthermore…..
”Safety of vaccines administered during pregnancy needs to be evaluated for both the mother and her newborn, and is an important consideration for the mothers' willingness to receive a vaccine during pregnancy. There is a significant bulk of evidence to support the safety of immunization with tetanus toxoids (TT), the longest standing vaccine that is recommended during pregnancy. (I think this claim is false given the studies listed above) There is also an increasing body of evidence to support the safety of pertussis and influenza immunization during pregnancy (see below specific sections). However, continuous assessment and reporting of adverse events after immunization during pregnancy remains important, especially for relatively newly introduced maternal vaccines (e.g., pertussis), as it informs about rare events that might follow immunization. In addition, assessment of baseline pregnancy outcomes in unvaccinated women in different world regions and settings will help in establishing baselines to assess safety outcomes against.
Furthermore, there is significant heterogeneity and lack of consensus on adverse event reporting in maternal immunization studies. This is a challenge for comparing and pooling data from different studies. In an attempt to overcome this weakness, WHO and the Brighton Collaboration worked together to provide written guidance on how to conduct safety studies in the field of maternal immunization (19). The initiative termed the Global Alignment of Immunization Safety Assessment in Pregnancy (GAIA) project worked on standardizing the assessment of safety of vaccines in pregnancy with specific focus on LMICs (20). Specifically, this initiative proposed systematic data collection, specific case definitions of key obstetric and neonatal health outcomes, ontology of key terms and a map of pertinent disease codes. More recently, case definition and guidelines for data collection, analysis and presentation has been proposed for neonatal seizures, neurodevelopmental delay, chorioamnionitis and post-partum endometritis and infection by the GAIA and Brighton collaboration working groups (21–24). Future studies assessing safety of immunization during pregnancy should use the proposed terms and definitions. In addition, currently available data on safety of vaccination in pregnancy is derived from vaccines that were initially licensed in non-pregnant populations. Future vaccine trials will likely assess vaccines intended to be licensed primarily for use in pregnant women. This further emphasizes the need to standardize reporting of safety outcomes in maternal immunization trials. Thus, we recommend following the GAIA and Brighton collaboration guidelines for assessment and reporting of safety outcomes in maternal immunization trials.”
This paper outlines the major issues in the metrics used to assess safety of vaccination during pregnancy including those specific to the pregnant body and infant. Hopefully these metrics include following the mothers and babies for more than a few weeks after birth, or even a full year. Many potential issues that arise may not manifest until the child is much older, and in the case of autism, the average diagnosis is 5 years old. Whats more, to put this in perspective, doctors seemingly know very little about the pregnant body insomuch as delayed cord clamping has to be part of the birth plan (if allowed at all) and is not part of basic protocol. 1/3 of the blood for the baby is in that placenta, and its treated as waste. Add this to the list of issues with birthing in the US, where doctors schedule births around golf schedules, and allow women to schedule inductions if they are past their due date. This study directly correlates c-sections with increased risk of immune issues in the child. The infant’s body and the pregnant body are both in a down regulated immune state. The mother, so she doesn’t reject the fetus, and the baby once born, so their immune system can learn slowly. Vaccination should be contraindicated for just those reasons alone.
I find it unscientific to vaccinate during pregnancy and it is clearly one big vast experiment affecting pregnant mothers and their unborn children where the full effects of this strategy to ‘eradicate disease’ is not assessed which should include expanding the potential side effects geared more toward typical vaccine injury rather than just pre-term birth and other typical congenital deformaties etc. It’s bad enough we have conventional vaccines to contend with. The mRNA experimental vaccines like the COVID jab and the new RSV injections are another level. Pharmaceutical companies stand to make billions off the relatively new marketability of vaccinations to pregnant women, where safety takes a back seat, like with all other vaccinations on the childhood schedule. And just like the childhood schedule, cumulative safety assessments have not occurred with the several vaccines pregnant women are receiving in their third trimester.
The vast amount of scientific research that can be search via PubMed regarding vaccinations and pregnancy will make your head spin, but once you start looking deeply into these studies you will quickly realize that the basis for safety AND efficacy is a shabbily built house of cards.
Sara Woods Kender
sara@sarasherbs.com
Clinical Herbalist
Reiki Master/Teacher
Psychic Medium
Munay-Ki Attuned
Find me on Substack!
Living In Circle

{kind=link}
IPAK-EDU Instructor & Affiliate
Use my code: HERBS1IPAK
https://ipak-edu.org/registration/
Click link for Educational Opportunities
Gaeta Institute
Nature First, Drugs Last
Click the link for 10% off tuition
https://michaelgaeta.teachable.com/?referral_code=G4IDF4
Sacred Tree Herbals
169 Daniel Webster Highway, Unit 1
Meredith, NH 03253
www.sarasherbs.com
Hours:
Wed-Saturday 9:30-4:30